







J. Cardiovasc. Dev. Dis. 2023, 10(8), 342; https://doi.org/10.3390/jcdd10080342 - 08 Aug 2023
Abstract
(1) Background. Obesity is a well-established worldwide recognised risk factor for atrial fibrillation (AF). Prior review papers reported on the associations between obesity and AF development, but not on the relation between obesity and atrial electrophysiology. We therefore conducted a systematic review to
[...] Read more.
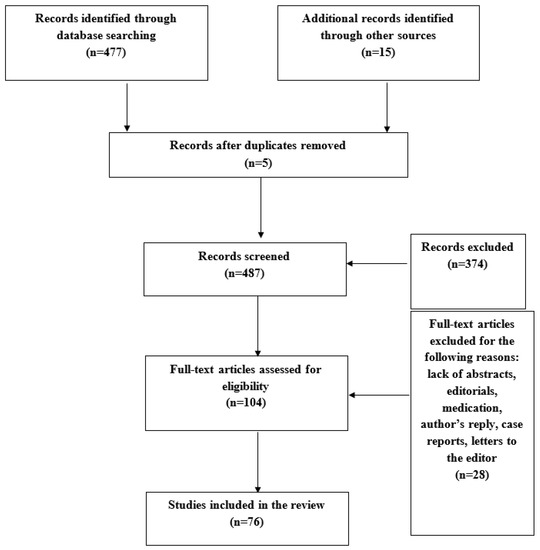
(1) Background. Obesity is a well-established worldwide recognised risk factor for atrial fibrillation (AF). Prior review papers reported on the associations between obesity and AF development, but not on the relation between obesity and atrial electrophysiology. We therefore conducted a systematic review to describe the current knowledge of the characteristics of the atrial electrophysiological substrate in obese individuals and how they relate to the development of AF. (2) Methods. A search was conducted in Pubmed, Embase, and the Cochrane Library for publications evaluating the impact of obesity on atrial electrophysiology, electrical substrates, and their relation to the development of AF. (3) Results. A systematic literature search retrieved 477 potential publications based on the inclusion criteria; 76 full-text articles were selected for the present systematic review. The literature demonstrated that obesity predisposes to not only a higher AF incidence but also to more extensive atrial electrophysiological abnormalities increasing susceptibility to AF development. (4) Conclusion. Obesity may predispose to an overall increase in atrial electropathology, consisting of an increase in the slowing of the conduction, conduction block, low-voltage areas, and complex fractionated electrograms. To determine the impact of obesity-induced atrial electrical abnormalities on the long-term clinical outcome, further prospective studies are mandatory.
Full article
(This article belongs to the Special Issue Electropathology as the Foundation of Innovation in Diagnosis and Therapy of Atrial Fibrillation)
►
Show Figures
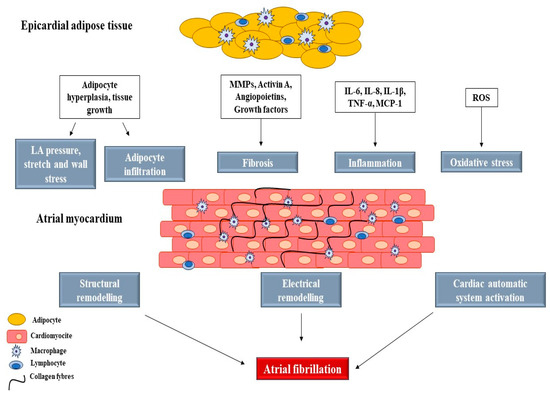
Figure 1


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}